The Checkpoint Inhibitor Revolution: Why the First Trials Changed Everything

In March 2011, the FDA approved a drug that would fundamentally change our understanding of cancer treatment forever. Ipilimumab (Yervoy), the first immune checkpoint inhibitor, represented more than just another cancer therapy—it was proof of concept that the human immune system could be unleashed to achieve durable, potentially permanent cancer cures. The early trials of checkpoint inhibitors didn’t just offer hope; they rewrote the rules of what was possible in oncology.
The Historical Context: A Desert of Failed Treatments
To understand the revolutionary nature of these early checkpoint inhibitor trials, we must first appreciate the landscape they emerged from Metastatic melanoma, where ipilimumab first proved its worth, was considered a death sentence. For the last 40 years, treatment advances had been largely stagnant. Traditional options for late-stage patients lacked substantial efficacy. These included IL-2, which showed only a 6 percent complete response rate1, and dacarbazine, which produced only a 6 percent to 15 percent response rate with no improvement in survival1
Patients with early Stage I lesions had high 3-year survival rates (more than 90 percent), but individuals with late-stage melanoma had a poorer prognosis (10 percent) with a median survival of only 7.5 months after diagnosis1. In this context of desperation, the emergence of checkpoint inhibitors represented the first glimmer of hope in decades.

The Breakthrough: Ipilimumab’s Revolutionary Results
The pivotal phase III trial that led to ipilimumab’s approval was nothing short of groundbreaking. The drug was the first treatment of any kind ever shown in a large, randomized phase III clinical study to improve overall survival in patients with metastatic melanoma who no longer respond to standard therapy2. Median overall survival was 10.1 and 10.0 months in the ipilimumab and ipilimumab plus vaccine arms, respectively, versus 6.4 months in the vaccine-alone group (hazard ratio, 0.68; P ≤ 0.003)3.
But the most remarkable aspect wasn’t just the improved survival—it was the durability of responses. Among 676 randomized patients, 94 (20%) and 42 (16%) survived ≥2 and ≥3 years, respectively4. Survival rates at 2 and 3 years were 25% (24 of 95) and 25% (13 of 53) with ipilimumab alone4. In a disease where survival was previously measured in months, patients were now living for years.
The Mechanism: Understanding How Checkpoint Inhibitors Work
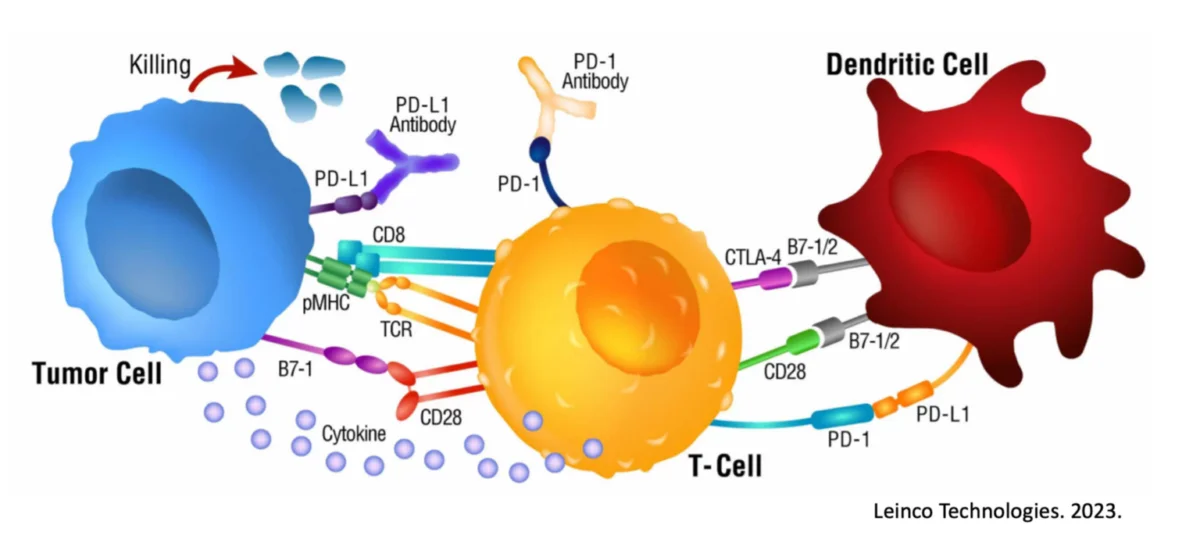
The revolutionary aspect of checkpoint inhibitors lies in their mechanism of action. Unlike chemotherapy or radiation, which directly attack cancer cells, checkpoint inhibitors work by removing the brakes on the immune system.
CTLA-4 is a receptor that normally functions to inhibit inappropriate or prolonged activation of T-cells5. Under certain conditions, T cells upregulate the cell surface molecule CTLA-4, which binds to B7.1 and B7.2 with greater affinity than does CD28. This series of events effectively hijacks signal 2, resulting in a situation in which specific T cells cannot be fully activated. Ipilimumab (and other anti-CTLA-4 antibodies) bind to CTLA-4 on the cell surface, effectively blocking the interaction between CTLA-4 and B7.1/B7.23.
Similarly, PD-1/PD-L1 checkpoint inhibitors work by blocking the binding between PD-1 (a checkpoint protein on immune cells called T cells that normally acts as a type of “off switch”) and PD-L1 (a protein on some normal and cancer cells)6. When PD-1 binds to PD-L1, it basically tells the T cell to leave the other cell alone. Some cancer cells have large amounts of PD-L1, which helps them hide from an immune attack6.

The Cascade of Success: PD-1/PD-L1 Inhibitors
The success of ipilimumab paved the way for the next generation of checkpoint inhibitors. Subsequently, two PD-1 antibodies, pembrolizumab (trade name Keytruda) and nivolumab (trade name Opdivo), developed by Merck and BMS respectively, obtained FDA approval7. Since then, immune-oncologic (I-O) drugs called immune checkpoint inhibitors (ICIs) have begun to be widely applied in various cancers7.
The PD-1/PD-L1 pathway inhibitors showed even more promising results than CTLA-4 blockade. Two phase 3 trials have shown superior efficacy of nivolumab, as compared with chemotherapy, in previously untreated patients with wild-type BRAF tumors or in patients with either mutant or wild-type BRAF tumors after progression during ipilimumab therapy8,9. These antibodies were associated with objective responses in 30 to 40% of patients, with the majority of responses being durable8,9.
The Profound Implications: Redefining What’s Possible
The early checkpoint inhibitor trials revealed something profound about cancer and the immune system that had previously been only theoretical: the immune system, when properly unleashed, could provide durable control of advanced cancer.
Long-Term Survival Curves
The most striking aspect of checkpoint inhibitor trials was the shape of their survival curves. Unlike chemotherapy, where survival curves typically showed steady decline, checkpoint inhibitor curves demonstrated a “tail”—a plateau where a subset of patients achieved long-term survival4. Approximately 20% of treated patients had long-term survival4. This pattern suggested that for some patients, checkpoint inhibitors weren’t just extending life—they were potentially providing cures.
The Power of Immunological Memory
These early trials demonstrated the concept of immunological memory in cancer treatment. When the immune system was properly educated to recognize cancer, it could provide lasting protection. This represented a fundamental shift from the traditional cancer treatment paradigm of repeated cycles of therapy to the possibility of a one-time intervention with lasting benefits.
Expanding the Treatable Population
As soon as November 2021, 8 ICIs were approved for 18 cancer types7, demonstrating the broad applicability of checkpoint inhibition across multiple tumor types. This universality suggested that immune recognition of cancer could be harnessed across diverse malignancies.

Permanent Limitations of Checkpoint Inhibitors
Despite their revolutionary impact, checkpoint inhibitors face significant inherent limitations that prevent them from benefiting all patients:
The PD-L1 Expression Barrier
Only 20–40% of patients derive benefit from these new therapies10. PD-L1, quantified using immunohistochemistry assays, is currently the most widely validated, used and accepted biomarker to guide the selection of patients to receive anti-PD-1 or anti-PD-L1 antibodies10. However, across all FDA approvals, PD-L1 was predictive in only 28.9% of cases, and was either not predictive (53.3%) or not tested (17.8%) in the remaining cases11.
The Fundamental Prerequisite Problem
One limitation to their use is that their activity is dependent on the generation of a population of T cells capable of recognizing the tumor through antigen-presenting cells (APCs)12. If this process does not occur, blocking PD-1/PD-L1 is inefficient, as there is a lack of immune response to unleash for the effective killing of the tumor cells12.
This represents the core limitation: checkpoint inhibitors can only remove the brakes from an immune response—they cannot create one where none exists.
Immunologically “Cold” Tumors
Many tumors exist in immunologically “cold” states with minimal T-cell infiltration13. Even for patients with tumors highly positive for PD-L1, more than 50% of them might not respond to PD-1/PD-L1 blockade13. Due to tumor heterogeneity and many other reasons, clinical responses vary largely across different tumor entities13.
Biomarker Limitations
Response rate of PD-1/PD-L1 inhibitors in overall patients is unsatisfactory, which limits the application in clinical practice14. Therefore, biomarkers which could effectively predict the efficacy of PD-1/PD-L1 inhibitors are crucial for patient selection14. Current biomarkers remain imperfect predictors of response15.

Biomarker Limitations
Immunocine’s personalized dendritic cell therapy addresses the fundamental limitation of checkpoint inhibitors by creating the very immune response that checkpoint inhibitors require to be effective.
Creating the Missing Link
While checkpoint inhibitors remove the brakes from existing immune responses, Immunocine’s approach creates the immune response in the first place. By using the patient’s entire cancer as a teaching tool through our “Double Loading” dendritic cell process, we educate the immune system to recognize cancer that it previously ignored through “immunological ignorance.”
The Educational Foundation
Our treatment establishes the prerequisite that checkpoint inhibitors need: a population of T cells capable of recognizing the tumor. By presenting the cancer’s complete mRNA and protein library to dendritic cells using our proprietary methodology, we create comprehensive immune recognition rather than relying on the limited, single-target approaches of other therapies.
Unlocking Checkpoint Inhibitor Potential
Most significantly, our treatment can potentially unlock the future use of checkpoint inhibitors in patients who were previously ineligible. Many of our patients see their cancers begin to upregulate PD-L1 as they start fighting off the newly educated immune response. This represents basic immunology: when cancer is finally under genuine immune attack, it upregulates defensive checkpoints like PD-L1.
This creates a unique opportunity: patients who complete our treatment and develop an active immune response against their cancer may become candidates for checkpoint inhibitors that would have been ineffective before immune education. We’re essentially lighting the fuse on an immune response, after which checkpoint inhibitors can be used to remove the brakes.
Beyond Biomarker Limitations
Our approach works regardless of initial PD-L1 expression, tumor mutational burden, or other current biomarkers because we’re creating a new immunological reality rather than relying on existing immune recognition. We’re not constrained by the tumor’s current immune profile—we’re changing it.

The Synergistic Future
The combination of Immunocine’s immune education with subsequent checkpoint inhibition represents a rational, mechanistic approach to cancer immunotherapy:
- First: Educate the immune system to recognize cancer (Immunocine)
- Then: Remove the brakes from that educated immune response (checkpoint inhibitors)
This sequential approach addresses both the limitation of checkpoint inhibitors (lack of initial immune recognition) and maximizes their potential (unleashing a properly educated immune response).
Conclusion
The early checkpoint inhibitor trials proved that the human immune system possesses the power to control and potentially cure advanced cancer when properly unleashed. These studies revealed that durable, long-term survival was possible through immune activation—something chemotherapy and radiation could never achieve.
However, the inherent limitations of checkpoint inhibitors—their dependence on pre-existing immune recognition and their restriction to PD-L1+ or biomarker-positive tumors—prevent many patients from benefiting from this revolutionary approach. Immunocine’s personalized dendritic cell therapy doesn’t compete with checkpoint inhibitors; it complements and enables them. By creating the immune recognition that checkpoint inhibitors require, we can potentially expand the population of patients who could benefit from the entire checkpoint inhibitor revolution.
The early checkpoint inhibitor trials showed us what’s possible when the immune system is unleashed. Now, through comprehensive immune education, we can ensure that more patients have an immune system capable of being unleashed in the first place. This represents not just the next evolution in cancer immunotherapy, but the fulfillment of the promise that those early revolutionary trials first revealed.
References
- Mansh, M. et al. Ipilimumab and cancer immunotherapy: a new hope for advanced stage melanoma. Yale J. Biol. Med. 84, 381-389 (2011).
- O’Donnell-Tormey, J. et al. FDA approves new immunotherapy for metastatic melanoma. Cancer Res. Inst. (2011).
- Hodi, F.S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363, 711-723 (2010).
- McDermott, D.F. et al. Efficacy and safety of ipilimumab in metastatic melanoma patients surviving more than 2 years following treatment in a phase III trial (MDX010-20). Ann. Oncol. 24, 2694-2698 (2013).
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 12, 252-264 (2012).
- American Cancer Society. Immune checkpoint inhibitors and their side effects. https://www.cancer.org/cancer/managing-cancer/treatment-types/immunotherapy/immune-checkpoint-inhibitors.html (2025).
- Lee, J.B. et al. Immune checkpoint inhibitors in 10 years: contribution of basic research and clinical application in cancer immunotherapy. Immune Netw. 22, e2 (2022).
- Larkin, J. et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med.373, 23-34 (2015).
- Brahmer, J. et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373, 123-135 (2015).
- Doroshow, D.B. et al. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat. Rev. Clin. Oncol.18, 345-362 (2021).
- Davis, A.A. & Patel, V.G. The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 7, 278 (2019).
- Han, Y. et al. PD-1/PD-L1 checkpoint signaling inhibition for cancer immunotherapy: mechanism, combinations, and clinical outcome. Front. Pharmacol. 8, 561 (2017).
- Yi, M. et al. Resistance to PD-1/PD-L1 blockade cancer immunotherapy: mechanisms, predictive factors, and future perspectives. Biomark. Res. 8, 35 (2020).
- Guerrero, J.M. et al. Melatonin and the immune system. Curr Opin Investig Drugs, 2, 696-699 (2001).
- Havel, J.J. et al. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat. Rev. Cancer19, 133-150 (2019).
READ THIS NEXT

Metformin + Losartan: Everyday Medicines That May Help “Warm Up” Cold Tumors for Immunotherapy
Many solid tumors are “cold”—fibrotic, poorly perfused, and hard for T cells to enter—so even breakthrough immunotherapies can stall
Read More
On Air with Immunocine: Matt Halpert Joins Heal Navigator to Discuss How the IDCT is Changing Lives Today
https://www.youtube.com/watch?v=SnFprB1I_K8&list=PLCaoz22dM92-Co9qqZESVpw-GNUdB0MV9 Listen to this Episode on Apple Podcasts Listen to
Read More
Team Spotlight: Susana Hernandez, MSc
Meet Susana Hernandez, Immunocine’s Director of Cell Therapy. Based in Cancun, Susana blends deep scientific expertise with a lifelong pas
Read More